What is corrected age?
When interpreting the different biological parameters in preterm children, it is necessary to bear in mind that their chronological age is not equivalent to that of the rest of the individuals.
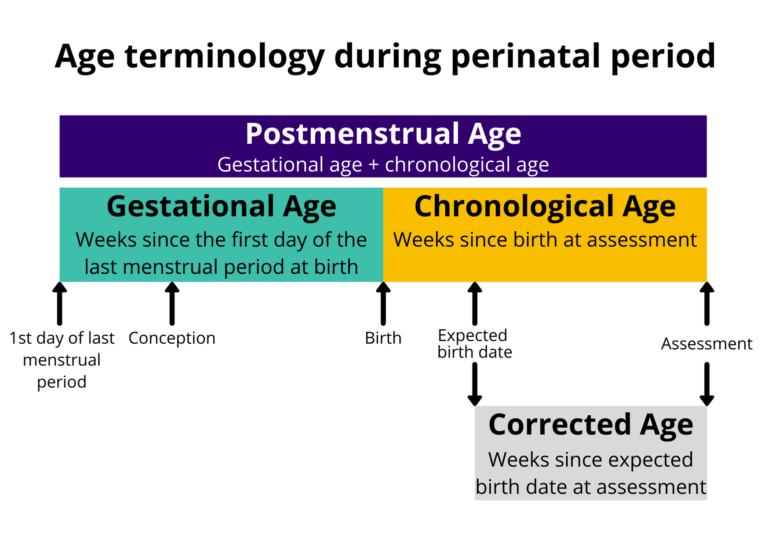
The concept of corrected age, arises as a way to infer the actual biological age the child would have if they had been born on their expected due date. It is calculated by subtracting the child's weeks of prematurity from their chronological age, which are calculated by subtracting the gestational age at birth from 40.
This allows us to compare a preterm child with the cohort of children born at term, and know whether their weight, height, and head circumference are consistent with their peers.
There are mobile applications to calculate corrected age quickly, such as the Edad Corregida app for Android.
Validity of corrected age.
However, this is a calculation that is based on a flawed premise, that the weeks of extrauterine life are equivalent to those of intrauterine life.
However, the reality is very different, as the extrauterine environment is adverse, the newborn loses placental nutritional support, and depending on the degree of prematurity, some of their organs/systems are not yet ready for autonomous life.
In general terms, from 2 years of age it is no longer necessary to correct age in a preterm child, since the distorting effect of prematurity decreases over time.
Corrected age and neurodevelopment.
On the other hand, transition to the extrauterine environment entails the onset of external stimuli that modify normal neurodevelopment, so that the development trajectory of a preterm baby will never be transferable simply by "changing" its date of birth.
Unfortunately, there are no specific developmental tests for the preterm population, so the best available approach remains the calculation of the equivalent age to compare them with the normal cohort.
Prematurity and early intervention. When to refer?
In any case, the decision to start early intervention must be based on two premises: acting is always better than not doing so, and if acting, it is better to act early.
For this reason, indications for early intervention do not depend only on the identification of a developmental delay in this subpopulation; the presence of risk factorsis very important, and these factors should be analyzed and stratified based on the probability of future neurodevelopmental problems (for example, preterm infants under 28 weeks of gestational age have an indication for stimulation regardless of their neurodevelopment).
All children who have neurodevelopmental problems, or are at risk of having them, will have a referral indication.