Cerebral palsy can be defined as a disorder of movement and posture control, which appears early and is the consequence of a lesion, malformation, or dysfunction of the central nervous system, and which is not the result of a progressive or degenerative brain disease.
- The problem can therefore appear pre-, peri-, or postnatally.
- The temporal criterion of the appearance of symptoms before 2 years of age (some authors say 5 years of age) is used as a cutoff point to differentiate cerebral palsy from acquired brain injury.
- A clinical follow-up must establish that it is not a progressive disease (although static encephalopathies can change the intensity of their symptoms depending on the stage of neurodevelopment, which is called pseudoregression).
- The neurological examination must establish that:
- It is a motor disorder (mainly, although there may be associated deficits).
- It is a disorder originating in the central nervous system (and neuromuscular diseases are excluded), which is inferred by the presence of clinical signs:
- Pyramidal.
- Extrapyramidal.
- The clinical history may be sufficient to establish a cause, although it is almost always necessary to use complementary tests, mainly neuroimaging, although genetic testing has gained special importance in cases without an established diagnosis.
The term cerebral palsy is therefore a descriptive term; it is not a single disorder but a set of different disorders with different etiologies, which nevertheless present in a stereotyped manner and share a series of characteristic complications.
Clinical presentations:
In outpatient clinics and primary care:
- In the follow-up of children "with risk factors", such as preterm infants.
- In children with motor development delay, particularly gross motor (sitting, standing, and walking).
- In children with asymmetric movement patterns, such as early hand preference.
- In children with muscle tone abnormalities, both hypotonia (early) and spasticity (late).
- In children with feeding problems, for example swallowing difficulties not explained by other medical causes.
In emergencies:
- Respiratory problems, particularly aspiration pneumonia.
- Poor control of epileptic seizures, including status epilepticus.
- Unexplained irritability: to consider acute infections, esophagitis, dental problems, hip subluxation, pathological fractures, constipation, adverse effects of pharmacological treatment, etc.
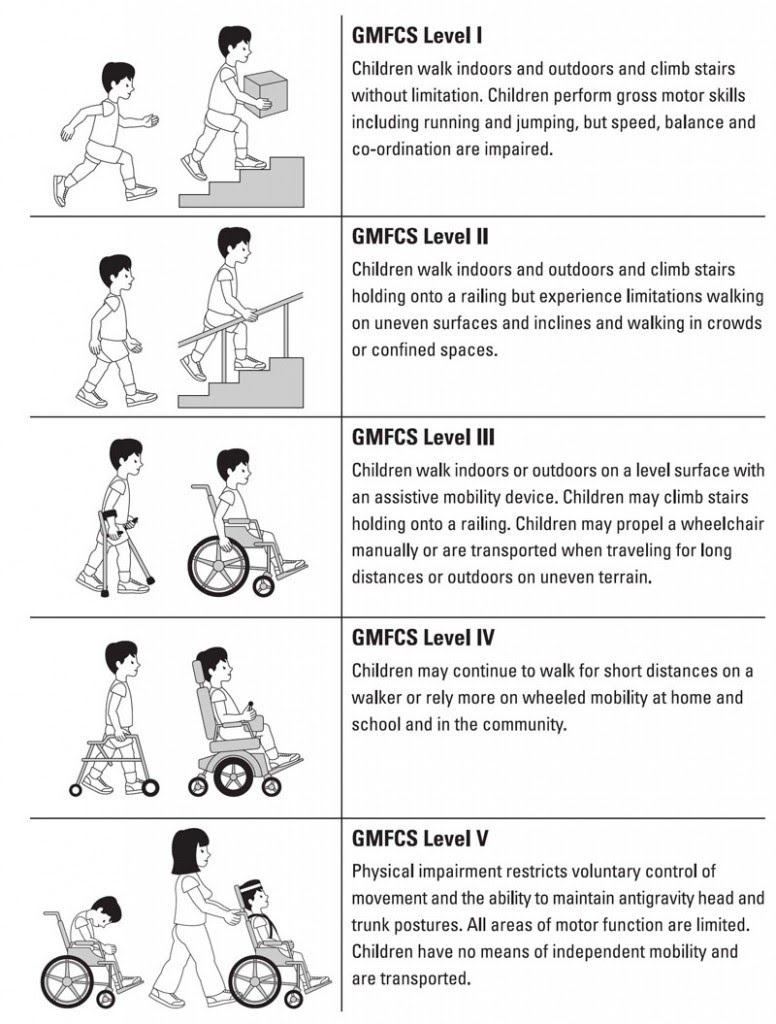
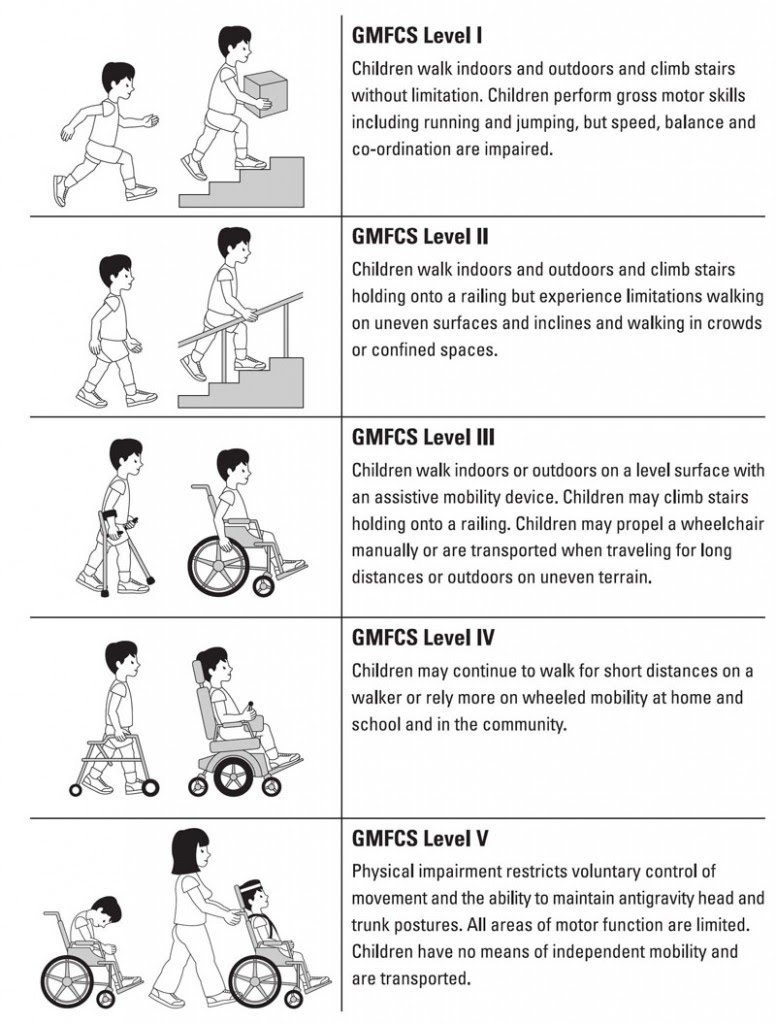
Stratification according to severity:
For severity stratification, the GMFCS (Gross Motor Function Classification System) is used.
Associated disorders:
Neurological comorbidity:
- Visual problems (up to 40%), such as strabismus, refraction problems, visual field defects, and cortical visual impairment.
- Hearing impairment (3-10%).
- Language and speech disorders.
- Epilepsy (50%).
- Cognitive difficulties, ranging from specific learning difficulties to intellectual disability.
- Spasticity.
- Sialorrhea.
- Urinary and/or fecal incontinence.
Other health problems:
- The growth and nutrition is a common problem in all cases; there are specific curves for this population group, based on their GMFCS and whether they are fed via gastrostomy or not.
- Motor disability leads to skeletal deformations secondary to immobility, spasticity, and the effect of gravity.
- Failure to thrive is very frequent, and it is necessary to use nutritional support strategies in many cases. In the most severe cases, feeding through a nasogastric tube or gastrostomy must be considered.
- On the other hand, overfeeding and obesity interfere with the development of motor skills and make care by caregivers more difficult.
- Gastrointestinal problems, such as gastroesophageal reflux and constipation.
- Some children with cerebral palsy develop chronic lung disease secondary to microaspirations as a consequence of oropharyngeal dysphagia or gastroesophageal reflux. It is necessary to monitor for coughing and choking during meals, as well as the appearance of wheezing after meals.
- Some children have a ventriculoperitoneal shunt, which must be monitored.
- Osteoporosis and even pathological fractures occur in the most severe cases.
- It is necessary to monitor dental health.
- Emotional problems are frequent.
- Orthopedic problems, such as contractures. They can develop over time, so orthotic treatment is very important. Sometimes they require surgical treatment.