Current status. Diagnostic substitution effect.
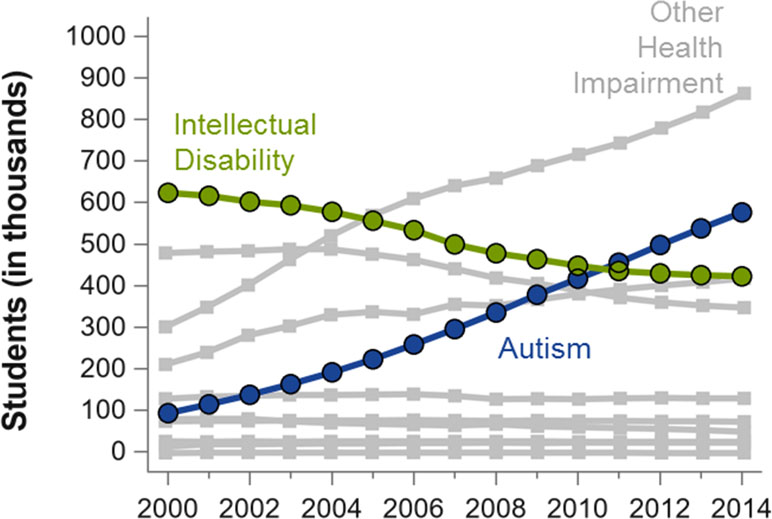
In recent decades, a process of diagnostic substitution has been occurring, with a progressive decrease in the use of the intellectual disability diagnosis and an increase in the ASD diagnosis. This is driven, among other reasons, by the increased sensitivity of professionals, as well as the search for early diagnosis of ASD (with the goal of diagnosing it between 18 and 24 months), which is not occurring in the case of intellectual disability, since its diagnostic criteria require individualized intelligence tests validated from 5-6 years of age.
Application of criterion E: Clinical guideline:
Clinical practice guidelines recommend the use of clinical judgment, over the use of specific algorithms or tests, for the differentiation between intellectual disability and autism spectrum disorder at any age. However, the following recommendations may be taken into consideration:
1. Having a quantitative cognitive and adaptive behavior assessment.
When evaluating an individual with intellectual disability for a potential ASD diagnosis, it is necessary to be aware of the child's actual cognitive ability (based on IQ, developmental quotients, or other developmental quantification) and to understand that these scores can be affected by causes unrelated to cognitive ability (the presence of a behavior disorder, for example). Therefore, it is recommended that the clinician responsible for the diagnosis directly administer the cognitive measurement test or have a detailed description of the individual's behavior during its administration. Correspondingly, the measurement of adaptive behavior will provide the context to interpret the clinical impact that the identified difficulties are producing globally.
2. The presence of other comorbid disabilities (visual, hearing, motor) that could affect cognitive assessment must be evaluated.
The evaluation of the presence of comorbid motor or sensory disability (vision, hearing, etc.) must be incorporated into the differential diagnosis, especially given the high frequency of simultaneous presentation of multiple disabilities in individuals with neurogenetic diseases and moderate or severe intellectual disability. If sensory disabilities exist, it is important to consider the use of validated tools for these specific populations (for example, specific developmental scales for blind children), and to consider a multidisciplinary evaluation that includes experts in those specific conditions.
3. Since criterion E requires that, for a comorbid diagnosis of ASD and ID, social communication skills must be below what is expected for the general developmental level, the evaluator must assess their ability to determine whether the observed deficits are consistent with what is expected for the child's developmental stage.
a. The expected behaviors at a certain developmental levelmust be considered. However, the child's chronological age is also relevant, since the effect of life experiences on behavior cannot be ignored. For example, the expected behavior of a child with a mental age of 18 months is different in a 4-year-old child or in an adolescent. As a result of more life experiences, the adolescent may be able to sit for longer periods, have more experience using certain devices or objects, and be more skilled in performing activities of daily living (training).
b. In the case of young children, DSM-5 warns that distinguishing intellectual disability from autism spectrum disorder is particularly difficult. At very early ages, it can be difficult or even impossible to determine whether there is a quantitative or qualitative problem (delay vs. deviation) in social communication skills, as asynchronous developmental profiles are more subtle when children are too young to have developed multiple skills.
c. In relation to the above, it is important to distinguish when symptoms are present but criterion E is not met, including when it is not possible to determine whether the symptom is present, absent or not applicable. For example, if there is a motor disability such as ataxia or motor apraxia that makes it impossible for the child to perform voluntary directed movements such as pointing, defining criterion E as “not applicable” better expresses the reason why the diagnostic criteria are not met. Likewise, it may not be possible to judge the presence or absence of certain symptoms in an individual who has not yet reached the level of development necessary for them to manifest, so the symptoms of autism may become apparent later.
4. In older individuals, the developmental trajectory can be particularly useful.
The clinician should specifically assess whether social communication skills have always been proportional to the other developmental domains, or if at times they have been the most significant difficulty. It is also important to take into consideration that the diagnosis of ASD can change over time. For example, as discussed above, it may not be possible to judge the presence of ASD in a child with very significant intellectual disability until they are able to develop a certain equivalent mental age. On the other hand, in cases of mild or moderate intellectual disability, evaluators should be cautious when assigning an ASD diagnosis at older ages in childhood, adolescence, or adulthood. It is unlikely that any individual (with or without intellectual disability) will suddenly manifest social communication deficits and repetitive and stereotyped behaviors beyond early childhood that are significant enough to qualify for an ASD diagnosis. In cases where this possibility is considered in an older individual with intellectual disability, it is necessary to consider whether the social communication difficulties identified are not simply a reflection of their social immaturity attributable to their intellectual disability, or potential changes in mental state in reaction to life transitions (for example, less social exposure after leaving school).
5. Application of specific screening and diagnostic tests for ASD.
Although the administration of ASD screening and diagnostic tests can be very useful in a wide variety of situations, the evaluator must first consider the consequences of the scaling and interpretation of the results. In both clinical and research contexts, the interpretation of results can be significantly limited in individuals with intellectual disability, ataxia, recent onset of walking, significant dysarthria or motor apraxia, and significant visual or hearing impairments. Therefore, although it is positive to try to rely on quantitative behavioral observations, the use of a particular tool can be problematic if it is not appropriate for the individual's abilities.
It is interesting to take into consideration that when autism-specific assessment tests are applied to individuals with well-defined genetic syndromes, a high frequency of autistic features is observed, but nevertheless, the diagnostic hypothesis of ASD had never been proposed. For example, the frequency of autism in Smith-Magenis syndrome, a disorder characterized by severe intellectual disability with multiple congenital anomalies, is up to 90%. About 63% of individuals with fragile X syndrome, one of the most common causes of intellectual disability, present characteristics of autism. About 93% of individuals with Williams-Beuren syndrome, a disorder characterized by severe developmental delay, also show autism symptoms.
6. When clinical judgment is applied, the evaluator's biases and motivations must be taken into account. The use of a multidisciplinary team can be very useful to allow for multiple observers and perspectives.
For clinicians who have a primary training in ASD, it may be necessary to seek significant support when dealing with individuals with certain medical, neurological, motor, or other problems, which are less common in individuals with ASD without intellectual disability. The evaluator must be aware that standardized tests perform differently in different populations, and that their own biases and idiosyncrasies, such as the relative weight they attribute to certain scores or observations, do not apply in the same way to all population groups. Furthermore, the evaluator must have sufficient information about the social history of the individual being evaluated, including family, sociocultural, and existing social support aspects, to evaluate the appropriateness of the primary caregiver's responses regarding the individual's ability to respond to different social situations.