We are evaluating a child with a neurodevelopmental disorder, in whom we suspect a genetic cause because they present suggestive findings (such as associated multiple congenital malformations). We have performed an aCGH which turned out to be normal. We have also performed a clinical exome (mendeliome) which has not provided us with conclusive information. Where do we go from here?
Re-evaluate variants of uncertain significance.
Review the appendices of the genetic report for relevant information.
The geneticist may have identified a pathogenic variant in a recessive gene, that is compatible with your clinical suspicion, but not finding a second pathogenic variant, they did not report it in the main body text. If the phenotype is consistent with the clinical suspicion, you may need to continue investigating:
Make sure there is no variant of uncertain significance on the other allele.
To confirm this, it is necessary to perform a parental segregation study; if both variants are found in trans, your suspected diagnosis will be strengthened.
Check for the existence of biomarkers.
If the autosomal recessive gene has biomarkers that allow its study, it can be an efficient strategy to perform a targeted study (enzymatic, biochemical) and, if abnormalities are detected, perform more sophisticated diagnostic tests (RNA sequencing) looking for deep intronic mutations.
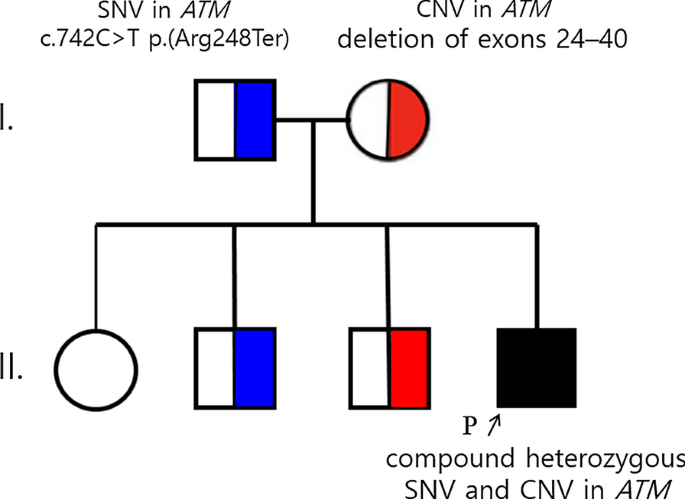
Consider the possibility of performing an MLPA of the affected gene.
Several mutational mechanisms may combine (compound heterozygosity), bear in mind that small deletions may have gone undetected in both tests (exome and aCGH).
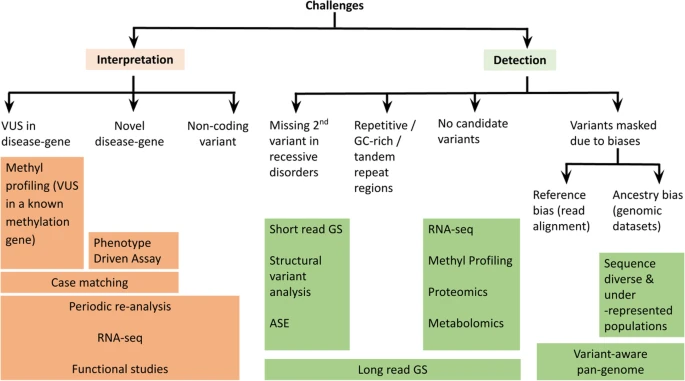
Review the possibility that it is a disease not diagnosable by sequencing.
There are some genetic diseases not diagnosable by exome sequencing with currently available technology. If the phenotype is compatible with any of them, it may be necessary to request specific diagnostic tests.
Re-evaluate the phenotype periodically in search of new orienting symptoms.
You can try to refine your phenotypic description using the HPO codes. This will make it easier for the geneticist to apply computer filters for data re-analysis.
With the phenotypic description using HPO codes, you can use computerized differential diagnosis tools, such as phenomyzer.
Ask your geneticist to re-analyze the raw sequencing data after 2-5 years if they have not done so automatically.
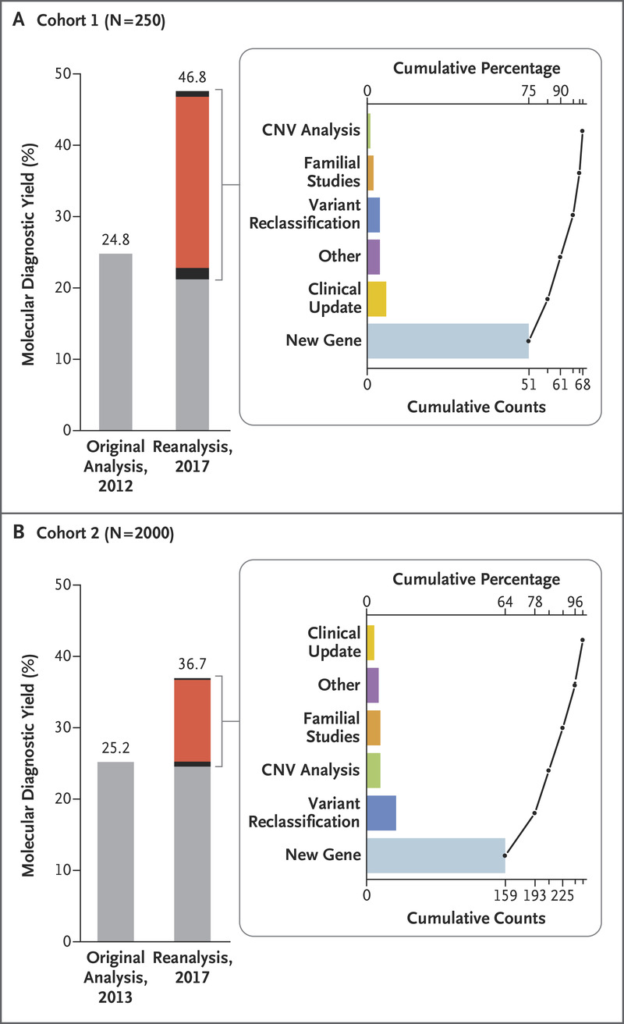
There are multiple scientific publications showing an increase of between 10-15% in diagnostic yield through the re-analysis of sequencing data 12-24 months after it was performed. This is a consequence of the rapid accumulation of scientific knowledge that is taking place:
- The discovery of new pathogenic genes.
- The clarification of the pathogenicity of variants not previously involved in disease.
- The refinement of population variants in the reference genome (Genome Reference Consortium).
- Segregation studies carried out in other families.
- Technical improvements in the application of filters in bioinformatics data processing (for example, the study of CNVs from sequencing data).
Consider the possibility of performing a trio exome sequencing (research).
The trio exome sequencing (index case, father, mother) allows crossing the data of the family members to apply filters that eliminate rare inherited genetic variants, in search of de novo variants in genes not yet fully studied that may be candidates to explain the phenotype. It is a technique that yields its greatest potential when systematically applied within the context of a research project, as it allows the discovery of new genes involved in disease and the demonstration of their pathogenicity through experimental techniques.
Start a collaborative network research with other professionals.
The Undiagnosed Diseases Network is a research network for undiagnosed diseases, in which professionals from several countries participate, and which acts as a facilitator in the research of rare diseases. There is a Spanish branch that depends on the ISCIII, and is called SPAINUDP.